D.C. District Court Strikes Down CMS’s Policy Divorcing the Rural Floor from the Rural Wage Index – On April 8, 2022, the United States District Court for the District of Columbia issued a decision setting aside CMS’s regulatory formula divorcing the calculation of the rural floor from the rural wage index. Citrus HMA, LLC v. Becerra, No 20-00707 (D.D.C. 2022). The plaintiffs, consisting of thirty-four hospitals from Arizona, Connecticut and Florida, alleged that CMS’s 2020 rural floor calculation, which assigned a rural floor that was lower than the rural wage index in that state, violates the statute’s command that the rural floor is the wage index “applicable” to rural hospitals. The District Court agreed, holding that the Medicare statute “unambiguously bars” CMS’s rural floor formula. King & Spalding represented the hospitals in the suit.
For the purposes of calculating the Medicare wage index, a hospital’s wages are generally counted in the area in which it is geographically located, but the Medicare statute contains an election that allows urban hospitals to be treated as if they were rural. This is known as rural reclassification. When a hospital makes this election, its wages and hours are included in the calculation of the rural wage index for its state. Thus, the rural wage index for each state is calculated based on the wage and hour data of all geographically rural and reclassified rural hospitals in the state.
The Medicare statute contains a safeguard to ensure that no urban hospital is assigned a wage index adjustment that is lower than the wage index that is “applicable” to rural hospitals in the state. This is known as the rural floor. This provision essentially means that an urban hospital is entitled to the greater of the wage index assigned to its home area or the one “applicable” to rural hospitals in the state in which it is located.
For decades, CMS considered the rural floor and the rural wage index to be one and the same. In the inpatient prospective payment system rule for Fiscal Year (FY) 2020, however, CMS devised a new methodology for calculating the rural floor. CMS continued to calculate the rural wage index for each state by including the wage and hour data of all geographically rural and reclassified rural hospitals within the state, but CMS calculated the rural floor separately, using only the wage and hour data of the geographically rural hospitals and excluding the data from reclassified rural hospitals. This change in policy produced rural floors that were significantly lower than the rural wage index in many states.
The plaintiff hospitals in Citrus HMA were urban hospitals that received wage index adjustments in FY 2020 that were well below the rural wage index values for their respective states. In their federal court briefings, the hospitals contended that CMS’s decision to calculate the rural floor separately from the rural wage index violated the statute because the rural floor provision says that the rural floor must be equal to the rural wage index.
CMS countered that the statute granted it discretion to calculate the rural floor separately from the rural wage index. The agency argued that there could be more than one wage index “applicable” to rural hospitals, and it was free to choose which one to use for calculating the rural floor. CMS also argued that the Medicare statute affords the agency wide latitude in calculating the wage index.
The District Court sided with the plaintiff hospitals, ruling that “the rural floor provision unambiguously provides that […] the rural floor and the rural wage index are one and the same.” The Court rejected CMS’s arguments, finding that “[n]othing in the statutory text supports [CMS’s] argument that [it] may calculate a rural wage index solely for purposes of determining the rural floor.” The Court further held that CMS’s general discretion does not license CMS to defy the unambiguous command of the rural floor provision.
The Court remanded the case back to CMS for further proceedings consistent with the Court’s decision. CMS has until June 7, 2022 to file an appeal with the United States Court of Appeals for the District of Columbia.
A copy of the District Court’s decision is available here.
Reporter, Alek Pivec, Washington D.C., +1 202 626 2914, apivec@kslaw.com.
CMS Finalizes Coverage Policy for Monoclonal Antibodies for the Treatment of Alzheimer’s Disease – On April 7, 2022, CMS released a national policy for the coverage of aducanumab (also known by the brand name Aduhelm) and any future monoclonal antibodies directed against amyloid approved by the FDA with an indication for use in treating Alzheimer’s Disease (AD). The finalized policy is available in a National Coverage Determination (NCD).
As previously reported, in January 2022, CMS released a proposed NCD memorandum which set forth the conditions under which Medicare would cover the use of monoclonal antibodies that target amyloid treatment for AD, which includes aducanumab, and accepted public comments on the proposed policy. In the press release announcing the finalized policy, CMS states that it reviewed more than 10,000 stakeholder comments.
Under the finalized NCD, CMS will cover FDA approved monoclonal antibodies directed against amyloid for the treatment of AD when furnished in accordance with specified coverage criteria under the Coverage with Evidence Development (CED) policy. The NCD limits coverage to patients who have a clinical diagnosis of mild cognitive impairment (MCI) due to AD or mild AD dementia, both with confirmed presence of amyloid beta pathology consistent with AD.
The NCD sets forth three circumstances under which Medicare will cover monoclonal antibodies directed against amyloid. First, Medicare will cover monoclonal antibodies directed against amyloid that are approved by the FDA for the treatment of AD when the drug is used in studies that meet certain CMS standards identified in the NCD (CMS approved studies). In this circumstance, the NCD allows for coverage of monoclonal antibodies that were previously approved by the FDA based upon evidence of efficacy as demonstrated by a direct measure in clinical benefit. Study data for these prospective comparative studies may be collected in a registry.
Second, Medicare will cover monoclonal antibodies that are approved by the FDA for the treatment of AD in a randomized controlled trial conducted under an investigational new drug (IND) application. The NCD allows coverage in this circumstance to monoclonal antibodies that receive approval based not on direct measures of clinical benefit, but upon evidence of efficacy as measured by a change in a surrogate endpoint (e.g., amyloid reduction) that is considered reasonably likely to predict clinical benefit.
Finally, the NCD specifies that monoclonal antibodies directed against amyloid indicated for the treatment of AD are covered when furnished according to the FDA approved indication when those drugs are used in National Institutes of Health (NIH)-supported trials.
Monoclonal antibodies directed against amyloid for the treatment of AD provided outside of a FDA approved randomized controlled trial, CMS approved studies, or studies supported by the NIH, are nationally non-covered.
For any CMS approved study, or NIH-supported trial, that includes a beta amyloid positron emission tomography (PET) scan as part of the protocol, it has been determined that these trials or studies also meet the CED requirements included in the Beta Amyloid Positron Emission Tomography in Dementia and Neurodegenerative Disease NCD (220.6.20).
CMS stated it is committed to continuing to explore ways to improve care for people with Alzheimer’s disease. The NCD is available here. A fact sheet on the policy is available here.
Reporter, Lauren Gennett, Atlanta, +1 404 572 3592, lgennett@kslaw.com.
CMS Issues Proposed Rules for Inpatient Psychiatric Facility and Inpatient Rehabilitation Facility Prospective Payment Systems for Fiscal Year 2023—On March 31, 2022, CMS issued proposed rules to update Medicare payment policies and rates for both the Inpatient Psychiatric Facility Prospective Payment System (IPF PPS) and the Inpatient Rehabilitation Facility Prospective Payment System (IRF PPS). CMS estimates that if finalized, both rules will result in an overall increase of payments to IPFs and IRFs and changes to the wage index calculation. The IRF proposed rule also contemplates changes to the teaching status adjustment and transfer policy.
Payment Rate Updates
As mentioned, CMS estimates that both proposed rules will result in increased Fiscal Year (FY) 2023 total payments for IPFs and IRFs respectively as compared to that which they received in FY 2022. Specifically, IPFs will receive an increase of 1.5% (or $50 million) in FY 2023 total payments, and IRFs an increase of 2% (or $170 million). Both proposed rules also delineate how CMS will achieve these increases by updating the IPF and IRF FY 2023 payment rates by 2.7% and 2.8% respectively. To accomplish this, CMS intends to update the IPF and IRF market baskets by 3.1% and 3.2% respectively, less a 0.4 percentage point productivity adjustment. If, however, more recent data becomes available, both the IPF and IRF proposed rules state that CMS will use the more recent data to determine the market basket update or productivity adjustment. Finally, both proposed rules include CMS’s plan to update the IPF and IRF outlier thresholds so that estimated outlier payments remain at 2% of total payments for IPF and 3% of total payments for IRF. CMS estimates that its proposal to the outlier threshold will result in a 1.2% overall decrease to aggregate payments for IPFs in FY 2023 and a 0.8 percentage point decrease in outlier payments for IRFs in FY 2023.
Consistent with its efforts to adjust Medicare payments to reflect accurately the cost of providing inpatient hospital and psychiatric services, CMS has solicited comments on its most recent IPF PPS refinement analysis.
Changes to Wage Index Calculation
In both the IPF and IRF proposed rules, CMS proposes to apply a 5% cap on wage index decreases for FY 2023 and subsequent years. This is an attempt to smooth year-to-year changes in a provider’s wage index and is consistent with similar changes that CMS made to the Inpatient Prospective Payment System (IPPS) starting in 2020.
IRF Teaching Status Adjustment
The IRF rule includes a proposal to codify CMS’s longstanding IRF teaching status adjustment policy and to clarify certain components of the same. CMS seeks public comment regarding the methodology used to determine facility-level adjustment factors and recommendations for what may cause the variability in the IRF teaching status adjustment.
IRF Transfer Policy
OIG recently recommended that CMS expand the IRF transfer payment policy to apply to early discharges to home health. To ensure that CMS strikes the appropriate balance between addressing patient needs and maintaining the integrity of the Medicare program, CMS seeks comments from stakeholders about implementing OIG’s recommendation.
CMS’s fact sheet for the IPF proposed rule is available here, and the agency’s fact sheet for the IRF rule is available here. The IPF proposed rule is available here, and the IRF proposed rule is available here.
Reporter, Sophie Munroe, Washington D.C., +1 202 626 5412, smunroe@kslaw.com.
CMS Issues Hospice Payment Rate Proposed Rule for FY 2023 — On March 30, 2022, CMS issued a proposed rule seeking to make routine updates to hospice-based payments and to the aggregate cap amount for FY 2023. CMS estimates that hospices will see a 2.7% ($580 million) increase in payments. Comments are due by May 31, 2022.
Payment Rate Update
CMS proposes a 2.7% hospice payment update for FY 2023, based on an estimated 3.1% inpatient hospital market basket update reduced by the productivity adjustment (0.4 percentage points). However, hospices that fail to meet quality reporting requirements will receive a 2-percentage point reduction to the annual market basket update for FY 2023.
This hospice payment update includes a statutory aggregate cap that limits the overall payments per patient for which CMS reimburses a hospice on an annual basis. The proposed cap for FY 2023 is $32,142.54—this is an increase of 2.7% ($31,297.61) over the FY 2022 cap amount.
CMS’s fact sheet for the hospice proposed rule is available here, and the hospice proposed rule is available here.
Reporter, Sophie Munroe, Washington D.C., +1 202 626 5412, smunroe@kslaw.com.
Federal No Surprises Act Online Independent Dispute Resolution Portal Opens This Week – Last week, CMS announced that the online Independent Dispute Resolution (IDR) portal will launch the week of April 11, 2022. Once the IDR portal is open, payors and providers will be able to submit disputes over out-of-network reimbursement through the portal. If the period for open negotiation has expired, the payors and providers have 15 business days following the opening of the IDR portal to submit a notice of initiation of the IDR process. The IDR process is used to determine the out-of-network rate payable by the plan when the No Surprises Act applies and there is no applicable specified state law in effect to determine the out-of-network rate.
If the payor and provider are unable to agree on a negotiated out-of-network rate during the open negotiation period, the parties will use the IDR process to resolve the dispute. The payor and provider will submit final offers for payment along with supporting materials to the IDR entity who is tasked with selecting between the two offers. The IDR is directed to consider the seven factors set forth in the No Surprises Act statute when determining the out-of-network rate, including: (1) the qualifying payment amount; (2) the provider’s quality, training, experience and outcomes; (3) the parties’ market share; (4) the complexity of the service and/or patient acuity; (5) the hospital’s case mix, teaching status, and scope of services; (6) previous contract rates over the past four years as well as each party’s good faith efforts to agree to a network contract; and (7) other credible and reliable information requested by or submitted to the IDR entity. The IDR entity is not permitted to consider the provider’s usual and customary rate or government program reimbursement rates.
As previously reported, the Eastern District of Texas granted the Texas Medical Association’s (TMA) motion for summary judgement. The TMA challenged portions of the No Surprises Act’s implementing regulations related to the IDR process. In the guidance that was struck down, the Departments made the Qualifying Payment Amount (QPA) the presumptive out-of-network rate. In light of the ruling, the IDR entity must now consider the seven factors outlined in the No Surprises Act (set forth above) when making the out-of-network rate determination and not make the QPA the presumptive out-of-network rate. CMS will issue revised guidance for payors and providers in light of this ruling.
CMS’s recent guidance about the No Surprises Act is available here. If you are interested in learning more about joining King & Spalding’s Price Transparency and Surprise Billing Working Group, please contact Amanda Hayes-Kibreab.
Reporter, Taylor Whitten, Sacramento, +1 916 321 4815, twhitten@kslaw.com.
HRSA to Reopen Provider Relief Fund Reporting for Certain Providers --The Health Resources and Services Administration (HRSA) will give certain recipients of payments from the Provider Relief Fund (PRF) another opportunity to comply with PRF reporting requirements. Between April 11, 2022 and April 22, 2022, providers may submit a request to report late if they can show an “extenuating circumstance(s)” that prevented compliance with the original reporting deadline. HRSA delineated what the agency will consider to be “extenuating circumstances.”
HRSA will consider the following to be “extenuating circumstances:”
-
Severe illness or death of a provider or key staff member responsible for reporting;
-
A natural disaster occurring during or in close proximity to the end of the reporting period causing the provider not to timely report;
-
The provider not receiving reporting communications due to an incorrect email or mailing address;
-
Failing to take the final step by clicking “Submit” on the report after registering and preparing a report in the PRF Reporting Portal;
-
Internal miscommunication or error regarding the individual who was authorized and expected to submit the report; or
-
An organization’s parent entity completing all General Distribution payments, but a Targeted Distribution(s) was not reported on by the subsidiary.
As previously reported, HRSA initially required recipients of PRF funds in excess of $10,000 to delineate their use of funds in a report submitted to HHS by September 30, 2021. On March 10, 2022, HHS sent notices to non-compliant providers instructing the providers that they had 30 business days to return the PRF funds.
HRSA will send written notification either approving or denying the request to report late. Providers who receive HRSA’s approval notice will have 10 days from the date they receive the notification to submit a report in the PRF Reporting Portal.
Providers who receive HRSA’s notification denying their request will remain non-compliant with the PRF requirements and will be required to return all funds to HRSA that were not reported in the applicable reporting period. Non-compliant providers will also be excluded from receiving and/or retaining future PRF payments.
More details on Requests to Report Late Due to Extenuating Circumstances are available on the HRSA website here.
Reporter, Nicholas Kump, Sacramento, +1 916 321 4817, nkump@kslaw.com.
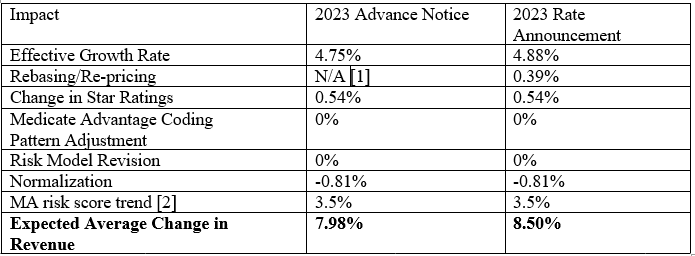
CMS Medicare Advantage and Part D Rate Announcement Includes Medicare Advantage Plan 8.5% Revenue Increase in 2023 – On April 4, 2022, CMS released the final 2023 Medicare Advantage and Part D rate announcement. CMS announced that Medicare Advantage plans’ revenue will increase 8.5% in 2023. This increase is larger than the 7.98% increase originally proposed in the February advance notice.
In explaining this rate increase, CMS noted that its “goals for Medicare Advantage and Part D mirror our vision for the agency’s programs as a whole, which is to advance health equity; drive comprehensive, person-centered care; and promote affordability and the sustainability of the Medicare program.”
The below chart published by CMS indicates the expected impact of the policy changes and updates on Medicare Advantage plan payments in 2022.
Year-to-Year Percentage Change in Payment
HHS Ends Temporary COVID-19 Emergency Blanket Waivers for Certain Providers –Reporter, Michelle Huntsman, Houston, +1 713 751 3211, mhuntsman@kslaw.com .
On April 7, 2022, HHS announced its intent to end temporary blanket waivers that the agency issued in response to the COVID-19 public health emergency (PHE) for three (3) specific provider types—skilled nursing facilities/nursing facilities (SNFs/NFs), inpatient hospices, intermediate care facilities for individuals with intellectual disabilities (ICF/IIDs), and end stage renal disease (ENRD) facilities. HHS implemented the waivers to relax certain federal regulatory requirements applicable to healthcare providers in order to allow providers the flexibility to respond to the COVID-19 PHE.
In its April 7 memorandum, HHS explained that it decided to terminate the COVID-19 PHE waivers for these particular providers based on its assessment of onsite survey information, which revealed that “the waiver of certain regulatory requirements has contributed” to “significant concerns with resident care unrelated to infection control” and “raises the risk of other issues.”
It is for this reason that HHS will terminate the PHE waivers for SNFs/NFs thirty (30) days from the date of the April 7, 2022 memorandum, or on May 7, 2022. The PHE waivers for ICF/IIDs and ENRD facilities will end sixty (60) days from the date of the memorandum, or on June 6, 2022. The April 7 memorandum makes clear that the temporary PHE waivers for hospitals and critical access hospitals will remain in effect.
HHS’s April 7 press release announcing the update to the COVID-19 PHE waiver for specific providers is available here, and the agency’s April 7 memorandum is here.
Reporter, Tamra Moore, Washington, D.C., +1 202 626 5458, tmoore@kslaw.com.
Ninth Circuit Affirms Dismissal of Out-of-Network Provider Lawsuit Against Medicaid Advantage Plan Based on Failure to Exhaust Medicare Program Administrative Remedies under 42 U.S.C. § 405 -- On April 8, 2022, the Ninth Circuit affirmed a district court order’s dismissal for lack of subject matter jurisdiction of an action brought by Global Rescue Jets, LLC, which sought recovery of amounts it had billed to an out-of-network Medicare Advantage Organization (MAO) under Medicare Part C.
An issue of first impression for the Ninth Circuit, the panel determined that an out-of-network provider seeking reimbursement from an MAO is required to exhaust the administrative remedies established by CMS under the Medicare Act in 42 U.S.C. § 405, prior to being able to file a lawsuit in court. Global Rescue Jets, LLC v. Kaiser Found. Health Plan, Inc., -- F.4th-- 2022 WL 1052671 (9th Cir. 2022).
Background Leading to this Lawsuit
In unrelated incidents, two patients who were enrolled in Medicare Advantage plans offered by Kaiser fell seriously ill while in Mexico and were unable to receive the care they needed there. Global Rescue Jets, which does business as Jet Rescue, provided emergency air ambulance services to transport the patients from Mexico to a Kaiser hospital in San Diego, California. According to Jet Rescue’s complaint, at the time of transport, both patients assigned their claims for benefits under Kaiser’s plans to Jet Rescue.
Jet Rescue did not have a contract with Kaiser for the services, so Jet Rescue billed Kaiser at its usual and customary rates: $283,500 for one patient, and $232,700 for the other. Kaiser refused to pay the billed amounts, taking the position that Jet Rescue’s air ambulance services would have been covered under original Medicare and thus were payable at the Medicare-approved rate, which Kaiser calculated as $23,096 for the first patient and $17,365 for the second.
Jet Rescue sought reconsideration directly from Kaiser as to one of the two enrollees. Kaiser denied the request for reconsideration. Jet Rescue did not seek further administrative review from Kaiser or CMS as to either enrollee. Instead, it sued Kaiser in state court to recover the additional sums for the services rendered, as the assignees of the beneficiaries.
Kaiser removed the action to federal court, asserting jurisdiction under the federal officer removal statute, 28 U.S.C. § 1442(a)(1), and under the federal question statute, 28 U.S.C. § 1331, on the theory that Jet Rescue’s claims arise under and are completely preempted by the Medicare Act. Jet Rescue contested these asserted bases for federal jurisdiction, but it did not move to remand, and instead amended its complaint to assert diversity jurisdiction.
Kaiser filed a motion to dismiss the First Amended Complaint under Federal Rule of Civil Procedure 12(b)(1). Kaiser argued that Jet Rescue’s failure to exhaust administrative remedies under the Medicare Act precluded the court from exercising subject matter jurisdiction.
The Ninth Circuit Held the Out-of-Network Providers’ Claims Were Subject to the Medicare Act
Rejecting Jet Rescue’s arguments to the contrary, the Ninth Circuit concluded that the claims asserted by Jet Rescue would constitute a payment of benefits under Part C of the Medicare Act; and thus, “arises under” the Medicare Act.
Jet Rescue first argued that the Medicare Act’s exhaustion requirements in 42 U.S.C. § 405 were inapplicable because: (1) an MAO is not an “officer or employee” of the United States or the Secretary of Health and Human Services (“HHS”); and (2) the lawsuit did not involve claims “arising under” the Medicare Act. The Ninth Circuit rejected those arguments, reasoning that MAOs must be officers or employees of the United States or the Secretary under § 405(h) for three reasons: (1) although private entities they also are an integral part of the administrative review scheme overseen by HHS and that Congress deemed MAOs, as the first-level reviewers of claims for benefits under Part C, to be “officers or employees” of the Secretary for purposes of § 405(h); (2) Congress created the multi-level administrative review scheme as a mandatory – not optional – requirement, which the Supreme Court affirmed; and (3) Congress’s imposition of a $1,000 amount-in-controversy requirement for judicial review would make no sense otherwise.
The Ninth Circuit also rejected the argument that the lawsuit did not involve claims “arising under” the Medicare Act. Quoting its reasoning in a patient benefits case, Do Sung Uhm v. Humana, Inc., 620 F.3d 1134 (9th Cir. 2010), a case brought by patients for benefits, the Ninth Circuit determined that “where, at bottom, a plaintiff is complaining about the denial of Medicare benefits,” the claim “arises under” the Medicare Act. Id. at 1142–43; cf. Ardary v. Aetna Health Plans of Cal., Inc., 98 F.3d 496, 500 (9th Cir. 1996) (holding that state law claims for wrongful death by a patient did not arise under the Medicare Act because they did not seek to recover benefits).
The Ninth Circuit also rejected Jet Rescue’s contention that emergency air ambulance services being a supplemental benefit rather than an original benefit made these services not arise under the Medicare Act. The Ninth Circuit concluded that it does not matter whether the benefit was supplemental or original because the authority of MAOs to offer supplemental benefits is derived entirely from Part C of the Act. See 42 U.S.C. § 1395w-22(a)(3).
The Out-of-Network Provider Had to Exhaust Administrative Remedies Here
The Ninth Circuit determined that Jet Rescue, an out-of-network provider, had to exhaust all of the available administrative remedies for these claims, pursuant to 42 U.S.C. § 405, before filing suit in court. The panel listed five separate administrative requirements before a lawsuit could be filed by a beneficiary under the Medicare Act to pursue a claim for benefits:
(1) an initial determination by the Medicare administrative contractor (MAC);
(2) a redetermination by the MAC;
(3) reconsideration by a qualified independent contractor (QIC);
(4) a hearing before an administrative law judge (ALJ) if the amount in controversy is $100 or more (adjusted for inflation); and
(5) review by the Medicare Appeals Council.
Global Rescue Jets, LLC, 2022 WL 1052671 at *4. If the beneficiary is dissatisfied with the Appeals Council’s decision, he or she may then seek judicial review, but only if the remaining amount in controversy is $1,000. Id. Jet Rescue had not attempted to use all five. There was no discussion in the opinion or issue raised by the parties addressing whether each of these five review levels were actually available at the time.
The Ninth Circuit determined the administrative review scheme under the Medicare Advantage program is modeled on the administrative review scheme Congress established for beneficiaries under original Medicare, and that pursuant to 42 U.S.C. § 405, original Medicare beneficiaries must exhaust their administrative remedies before seeking judicial review of a claim for benefits. The court panel found no basis for creating a different rule with respect to administrative exhaustion under the Medicare Advantage program. Accordingly, the panel held that the administrative exhaustion requirement imposed by Medicare Part C includes: (1) a non-waivable “presentment” requirement; and (2) a waivable requirement that enrollees pursue a claim for benefits through each available level of administrative review. Jet Rescue had met the first of these requirements but not the second, and, as it was suing in the capacity of an assignee of the enrollees for purposes relevant here, it therefore failed to exhaust administrative remedies.
The Out-Of-Network Provider Did Not Show that It Was Excused from Exhausting the Multi-Level Administrative Review Process Here
The Ninth Circuit rejected Jet Rescue’s contention that the exhaustion requirement should be excused here, but did confirm that it could be excused if three conditions had been satisfied: (1) the plaintiff’s claim is wholly collateral to a claim for Medicare benefits; (2) the plaintiff has made a colorable showing of irreparable harm; and (3) exhaustion would be futile. The panel concluded that Jet Rescue failed to meet its burden of proof on the first and third requirements.
As to the first requirement, a claim is deemed “collateral” in this context when it “is not bound up with the merits so closely that the court’s decision would constitute interference with agency process.” See Johnson v. Shalala, 2 F.3d 918, 922 (9th Cir. 1993) (internal quotation marks and brackets omitted). The Ninth Circuit determined that the issue of proper payment for Jet Rescue’s services is the subject of an organization determination that is final unless and until it is reviewed by the agency. See 42 C.F.R. § 422.576. Excusing exhaustion of administrative remedies would interfere with the agency’s opportunity to review those claims.
As to the third requirement, because administrative review would serve the purposes of exhaustion by allowing the agency to apply its expertise and assemble the relevant record, the panel found that such review would not have been futile. See Kaiser v. Blue Cross of California, 347 F.3d 1107, 1115 (9th Cir. 2003).
Out-of-Network Providers May Want to Engage in the Administrative Review Process to Either Recover through that Process or Establish Futility of the Process, Whether through A Test Claim or Multiple Test Claims
The multi-level administrative review process outlined by the Ninth Circuit places an onerous burden on any out-of-network provider seeking reimbursement from a Medicare Advantage plan via an assignment of benefits. However, an out-of-network provider may want to engage in that process to avoid what happened to Jet Rescue. This otherwise burdensome process has at least two potential benefits to an out-of-network provider. First, perhaps the provider will succeed at one of the administrative levels. Second, going through the process could help establish futility.
The Ninth Circuit recognizes that the administrative review is intended to allow the agency to apply its expertise and assemble the relevant record on disputes over benefits. See Kaiser v. Blue Cross of California, 347 F.3d 1107, 1115 (9th Cir. 2003). But once the relevant record is assembled and the agency has considered the claim, it becomes easier to argue futility on similarly situated claims, since it arguably would no longer provide value to any of the parties, including the administrative adjudicators throughout the appeals process, to repeat the exhaustion exercise.
Furthermore, this might be something that can be established through a test claim, or multiple test claims, depending on the circumstances. Whether one or more test claims makes sense depends on the specific factual situation. This is especially true for administrative appeals to CMS, as CMS’s administrative appeals programs are already burdened with a large, growing docket, and may reveal themselves as futile for appeals by out-of-network providers.
Attempting to utilize the administrative process also might establish futility if one or more steps contemplated by the Ninth Circuit do not actually exist in the real world when attempted. For example, the Medicare Advantage plan and/or CMS might not be operating one or more of the steps at the time the provider attempts the appeals. A nonoperating process is another method of supporting a futility argument to get an administrative process requirement excused.
Contracted Providers Would Likely Have Had a Different Result Because the Contract Creates a Different Source of the Right to Payment that Is Not Preempted by Medicare
A number of courts have distinguished the situation for contracted providers, determining that, where a contracted provider seeks payment from a Medicare Advantage plan, the claims for payment under the private contract do not arise under the Medicare Act and, therefore, are not subject to the exhaustion requirement.
For example, in RenCare, Ltd. v. Humana Health Plan of Texas, Inc. et al., 395 F.3d 555, 559-560 (5th Cir. 2004), the Fifth Circuit explained that a dispute between an in-network contracted provider and a Medicare Advantage plan is solely between the two private parties that contracted for benefits. The RenCare opinion found that contracted claims are not at all “intertwined, much less ‘inextricably intertwined,” with a claim for Medicare benefits, and thus, to the claims did not arise under the Medicare Act and exhaustion of remedies was not required. Id. at 559.
Likewise, in CHRISTUS Health Gulf Coast v. Aetna, Inc., 237 S.W.3d 338 (Tex. 2007), the Texas Supreme Court concluded that hospitals did not need to exhaust administrative remedies to assert a claim against a Medicare Advantage Plan that concerned payment for indisputably covered services.
Similarly, in Liberty Dialysis-Hawaii LLC v. Kaiser Foundation Health Plan, Inc., 2017 WL 4322385 (D. Hawai’i Sept. 28, 2017), the Hawaii District Court – which is within the Ninth Circuit – confirmed that the contracted provider was not required to exhaust administrative remedies and the dispute did not arise under the Medicare Act, explaining:
The test requires that a claim be “inextricably intertwined” with a claim for benefits before the exhaustion requirement applies. And where, as here, a claim for payment may be determined entirely by reference to a private contract, and requires no analysis or application of the Medicare Act, policies, or regulations, no consideration of plan documents or benefits, and no redetermination of a benefits decision, it simply cannot be said to be “inextricably intertwined” with a claim for Medicare benefits.
Id. at *5. See also Sarasota Cty Public Hosp. Bd. v. Blue Cross and Blue Shield of Fla., Inc., 511 F. Supp. 3d 1240 (M.D. Fla. Jan. 5, 2021) (denying a motion to dismiss because the contracted provider’s claims against the Medicare Advantage plan did not arise under the Medicare Act, concluding that the provider did not have to exhaust administrative remedies to bring suit).
The Eleventh Circuit specifically recognized the distinction between contracted and noncontracted providers in Tenet Healthsystem GB, Inc. v. Care Improvement Plus South Central Insurance Co., 875 F.3d 584 (11th Cir. 2017). In Tenet, the Plaintiffs were a group of hospitals, all “noncontract providers,” who had treated defendant's Medicare Advantage enrollees after receiving authorization to do so from the Medicare Advantage plan. Id. at 588. The court determined that the hospitals’ claims did “arise under” Medicare, because the hospitals were suing as “assignees of Medicare Part C benefits” and therefore “subject to the Medicare Act’s exhaustion requirements.” Id. at 590 (quotation marks omitted). In reaching this determination, however, the court emphasized the “critical” distinction between claims for payment made by contract versus noncontract providers against a Medicare Advantage plan, stating: “In billing disputes between MAOs and contract providers, the provider is pursuing a claim for reimbursement that only ever belonged to itself—the claim that arose under the express terms of its contract with the MAO.” Id. at *590 (quotation marks omitted). Citing RenCare, it explained that unlike claims brought by noncontract providers “[a] contract provider’s claims are determined entirely by reference to the written contract, not the Medicare Act.” Id. at *5. The court distinguished RenCare from the case before it stating, “[a]s the Ren[C]are court noted, the Medicare Act explicitly allows contract providers and MAOs to define the terms of their own agreements without reference to the Medicare regulations.” Id.
The Sixth Circuit went one step further in Ohio State Chiropractic Assoc. v. Humana Health Plan Inc., 647 Fed. App’x 619, 625 (6th Cir. 2016), suggesting in dicta, but not addressing, that RenCare’s reasoning might also apply to disputes between an MAO and noncontract providers.
Notably, the federal government has agreed that contracted providers do not need to use the Medicare administrative review process. HHS’s regulations provide an administrative review process that focuses on enrollees, not health care providers, and is designed to protect enrollees’ rights to Medicare benefits. See 42 U.S.C. § 1395w-22(g); 42 C.F.R. §§ 422.560-422.622. Further, HHS has filed amicus briefs in support of the position that requiring providers to exhaust administrative remedies would turn the administrative appeals process on its head. See CHRISTUS Health Gulf Coast v. Aetna, Inc., No. 05-0710, 2006 WL 985225, at *10-11 (Tex. filed Mar. 13, 2006) (“administrative exhaustion is not required when the “‘enrollee has absolutely no interest’” in the dispute.”); see also Ltr. Br. of United States 9, No. 15-3130, Ohio State Chiropractic Ass’n v. Humana Health Plan, Inc., (6th Cir. filed Mar. 14, 2016) (in a dispute involving a non-contracted provider, HHS stated that the “mandatory administrative review process does not extend to . . . [provider-MAO disputes] in which ‘Medicare beneficiaries were not denied services or reimbursement for services’ by an MAO.”) (quoting RenCare, 395 F.3d at 558).
The Ninth Circuit in the Jet Rescue case knew about the distinction between contracted and noncontracted providers, noting that the court did not need to decide whether a different conclusion would be warranted in a case involving a contract provider, citing RenCare. See Global Rescue Jets, LLC, 2022 WL 1052671 at *7, n.4. Thus, it is reasonable to conclude that a contracted provider, with claims arising under a privately negotiated contract which was not merely a promise to comply with the Medicare Act, would have had a different result in the Ninth Circuit than the experience of Jet Rescue.
The Ninth Circuit opinion is available here.
Reporters, Sara Brinkmann, Houston, +1 202 626 5458, sbrinkmann@kslaw.com and Glenn Solomon, Los Angeles, +1 213 443 4330, gsolomon@kslaw.com.
ALSO IN THE NEWS
CMS Delays Start Date of Medicare Payment Model for Cancer Patients – In a proposed rule released on April 6, 2022, CMS proposed to delay the current start date of the Radiation Oncology Payment Model to a date to be determined through future rulemaking. The model would bundle payments for radiation therapy provided to patients in various settings. The proposed rule is available here. King and Spalding’s reports on a previous decision by CMS to delay implementation of the Radiation Oncology Payment Model are available here and here.
HHS Requests Input Regarding How It Should Take into Account a Provider’s History of Compliance with Cybersecurity Measures – Under a 2020 law, the HHS Office of Civil Rights (OCR) is required to consider a provider’s security practices when considering the outcomes of audits and the amount of financial penalties it imposes. This requirement has not yet been implemented through rulemaking, and OCR has requested stakeholder input by issuing an RFI. The agency is also seeking comment regarding potential compensation to victims through recoveries. The RFI is available here.
A similar result occurred in a decision from the Eleventh Circuit. Tenet Healthsystem GB, Inc. v. Care Improvement Plus South Central Insurance Co., 875 F.3d 584, 588 (11th Cir. 2017) (holding that the out-of-network providers there seeking to recover payment from a Medicare Advantage organization were required to exhaust administrative remedies before filing suit).