OIG Issues Favorable Advisory Opinion Concluding Bonuses to Employed Physicians Are Not Kickbacks
Earlier this month, OIG issued Advisory Opinion 23-07, a favorable opinion regarding an employer’s proposal to pay bonuses to its employed physicians based on net profits derived from certain procedures performed by the physicians (the Advisory Opinion). As discussed in further detail below, OIG found that although the proposed bonus compensation arrangement would implicate the federal Anti-Kickback Statute (AKS), the proposed arrangement would be protected by the statutory exception and regulatory safe harbor for bona fide employees.
The Request
The Advisory Opinion was requested by a multi-specialty physician practice (the Requestor) that has approximately eleven physician employees (the Physician Employees), all of whom the Requestor certified are bona fide employees. Under the proposed arrangement, the Requestor proposes to implement an employment compensation bonus methodology for each of the Physician Employees, in addition to their base employment compensation, which would be in exchange for the services they provide on behalf of the Requestor, including services for which payment may be made under federal healthcare programs. Specifically, when a Physician Employee performs outpatient surgical procedures at either of two ambulatory surgical centers (ASCs) operated by Requestor in a given calendar quarter, the Physician Employee would receive a bonus equal to thirty percent of Requestor’s net profits from the ASC facility fee collections attributable to that physician’s procedures performed at the ASC for that quarter.
OIG’s Advisory Opinion
In the Advisory Opinion, OIG explained that when the relevant ASC procedures are referred by the Physician Employee and are reimbursable by federal healthcare programs, the AKS would be implicated. However, OIG ultimately concluded that the bonus compensation would be protected by the statutory exception and regulatory safe harbor for bona fide employees because:
- the Requestor certified that the Physician Employees would be bona fide employees of Requestor in accordance with the definition of that term set forth at 26 U.S.C. § 3121(d)(2); and
- the bonus compensation would constitute an amount paid by an employer to an employee for employment in the furnishing of any item or service for which payment may be made in whole or in part under Medicare, Medicaid, or other federal healthcare programs.
The Advisory Opinion notes that a similar arrangement involving bonus payments to independent contractor physicians or other nonemployees or under a different corporate structure may raise fraud and abuse concerns under the AKS. Indeed, the Fourth Circuit Court of Appeals has already twice held that commission-based compensation arrangements with independent contractors cannot be safe harbored and do violate the AKS and the federal False Claims Act (FCA). See, e.g., United States ex rel. Nicholson v. MedCom Carolinas, Inc., 42 F.4th 185 (4th Cir. 2022); and United States v. Mallory, 988 F.3d 730 (4th Cir.), cert. denied sub nom. Dent v. United States, 142 S. Ct. 485 (2021).
Advisory Opinion 23-07 is limited in scope to the proposed arrangement and cannot be relied upon by anyone other than the Requestor. However, the Advisory Opinion provides a helpful indication of how OIG might respond to similar requests. A copy of the Advisory Opinion is available here.
Reporter, Ahsin Azim, Washington, D.C., + 1 202 626 5516, aazim@kslaw.com.
New California Law Raises Minimum Wage for Health Care Workers Beginning June 1, 2024
On October 13, 2023, California Governor Gavin Newsom signed California Senate Bill No. 525 (SB 525) into law, which gradually raises the minimum wage to $25 for California health care workers.
Covered Health Care Facility Employers and Health Care Services
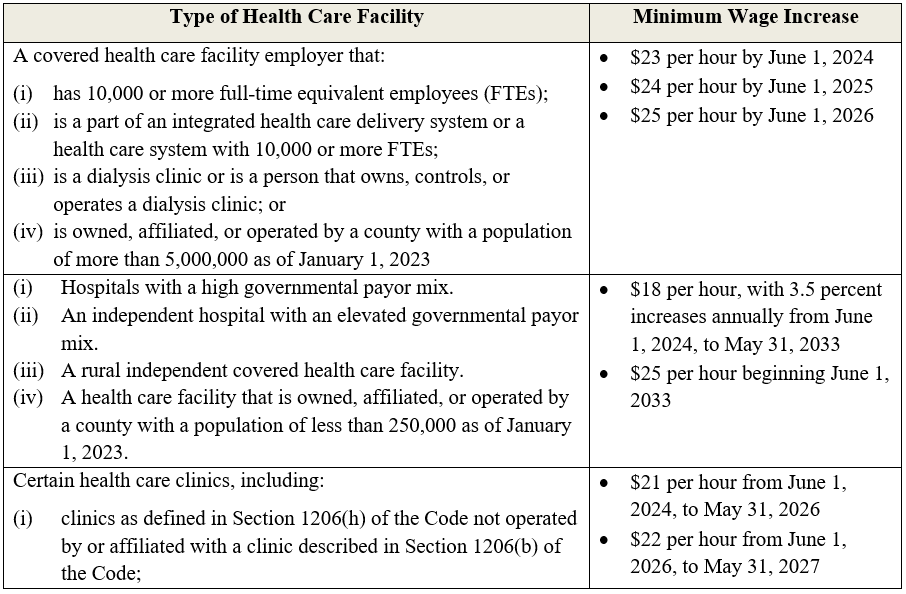
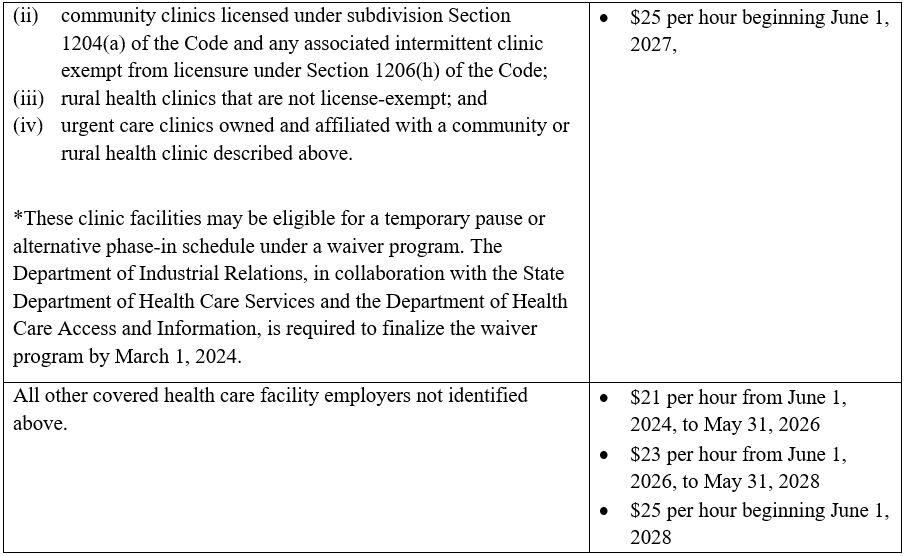
Beginning June 1, 2024, SB 525 requires most health care facilities to raise minimum wages for their employees, with the rate of the wage increases depending on the type of facility. Unless expressly exempted, facilities providing health care services must comply with the minimum wage increases under SB 525. The term “health care services” is defined broadly to mean “patient care-related services including nursing; caregiving; services provided by medical residents, interns, or fellows; technical and ancillary services; janitorial work; housekeeping; groundskeeping; guard duties; business office clerical work; food services; laundry; medical coding and billing; call center and warehouse work; scheduling; and gift shop work; but only where such services support patient care.”
SB 525 covers a broad range of health care facilities, including but not limited to (i) hospitals, (ii) clinics, (iii) home health agencies, (iv), psychiatric health facilities, (v) skilled nursing facilities if owned, operated, or controlled by a hospital or integrated health care delivery system or health care system and (vi) residential care facilities if affiliated with an acute care provider or owned, operated, or controlled by a general acute care hospital (or parent entity), acute psychiatric hospital (or parent entity). Exempt facilities include (i) hospitals owned, controlled, or operated by the Department of State Hospitals, (ii) tribal clinics exempt from licensure under Section 1206(c) of the Health and Safety Code (Code), and (iii) outpatient settings conducted maintained, or operated by a federally recognized Indian tribe, tribal organization or urban Indian organization, as defined in 25 U.S.C. 1603.
Covered Employees
SB 525 applies to the following types of workers:
- an employee of a health care facility employer who provides patient care, health care services, or services supporting the provision of health care (e.g., nurse, physician, caregiver, medical resident, intern or fellow, patient care technician, janitor, housekeeping staff person, groundskeeper, guard, etc.);
- a contracted or subcontracted employee if (i) the employee, contractor or subcontractor’s contracts with the health care facility employer to provide health care services, or services supporting the provision of health care and (ii) the healthcare facility employer directly or indirectly, or through an agent or any other person, exercises control over the employee’s wages, hours or working conditions; and
- all employees performing contracted or subcontracted work primarily on the premises of a health care facility to provide health care services or services supporting the provision of health care.
Mandated Increases to Minimum Wages
Depending on the type of health care facility, SB 525 provides for the following minimum wage increases:
SB 525’s full text is available here.
Reporter, Dennis Mkrtchian, Los Angeles, + 1 213 218 4046, dmkrtchian@kslaw.com.
California Revises Proposed Rules for Healthcare Transaction Filings
The California Office of Healthcare Affordability (OHCA) released updated regulations this month pertaining to the healthcare transaction notice requirements that will apply to transactions that close on or after April 1, 2024. The revised healthcare notice requirements incorporate several public comments that were submitted earlier this year.
Background
On June 30, 2022, the Health Care Quality and Affordability Act (SB 184) was signed into law in California. The new law established OHCA and set forth that OHCA would be tasked with overseeing and containing healthcare spending in California. As part of that responsibility, OHCA would review certain proposed healthcare transactions in the state.
Earlier this year, OHCA published proposed regulations to govern the review of proposed healthcare transactions that close on or after April 1, 2024. Beginning on April 1, 2024, a “health care entity” (defined below) is required to provide written notice to OHCA at least 90 days prior to entering into a covered agreement or transaction. Within 60 days, OHCA will advise the entity whether OHCA will conduct a cost and market impact review (CMIR) or provide a written waiver. OHCA must conduct a CMIR if the proposed transaction is “likely to have a risk of a significant impact on market competition, the state’s ability to meet cost targets, or costs for purchasers and consumers.”
OHCA may not block a transaction, but the review could take longer than the 90-day notice period and should be factored into a transaction’s closing timeline. If OHCA conducts a CMIR, the transaction may not close until 60 days after OHCA issues its final report. In addition, OHCA will make all materials submitted during the review publicly available unless the submitter files a request for confidentiality that is granted by OHCA.
Revised Regulations
The revised regulations make several key changes to the new notice requirements including:
- “Health Care Entity” Definition: The definition of “health care entity” includes any payer, provider, or fully integrated delivery system that would include physician organizations, hospitals, hospital outpatient departments, and ambulatory surgery centers. The updated regulations revise the definition of a health care entity to remove management services organizations (MSOs). However, the definition includes “an organization that acts as an agent of a provider(s) in contracting with payers, negotiating for rates, or developing networks.” Therefore, some MSOs may still be subject to the notice requirements if they act in this capacity.
- “Material Change Transaction” Definition: Only certain transactions are subject to the notice requirements. The revised regulations remove certain transactions from the notice requirements, including transactions that occur in the ordinary course of business and certain corporate restructuring transactions.
- Material Change Transaction Criteria: Under the revised regulations, the entities that are required to file a written notice of the transaction with OHCA include:
- Health care entities that have at least $25 million in revenue and control or own at least $25 million worth of California assets;
- Health care entities that have a least $10 million in revenue and control or own at least $10 million worth of California assets and are involved in a transaction with a health care entity that meets either of the $25 million thresholds described above; and
- Health care entities that are “located in a designated mental health or primary care health professional shortage area.”
- Material Change Thresholds: The updated regulations change some of the material change threshold notice triggering amounts, including revising the transaction amount from 20% to “25% or more of the total California assets of any health care entity in the transaction.” This revision raises the threshold amount and limits it to California assets instead of assets in general. The revised regulations also increase the threshold for transfer of control from 10% to “25% or more of the voting power of the members of the governing body of a health care entity.” If the transaction is a series of related transactions, the transactions will be treated as one transaction for purposes of meeting the thresholds described above. If those thresholds are met, the series of related transactions will be subject to the notice requirements.
- Expedited Review: The updated regulations add a new section setting forth guidelines for requesting an expedited review. The submitter will file the notice and the request for expedited review to OHCA at the same time. The request should include a description and documentation explaining why an expedited review is necessary and a date by which the submitter is requesting that the review be completed. Reasons for submitting an expedited review include severe financial distress or “any significant reduction in the provision of critical health care services within a geographic region or regions.” OHCA has discretion to deny a submitter’s expedited review request.
These revised regulations provide clarity on what types of entities and transactions are required to comply with these notice requirements. The updated rules also provide for a new expedited review, but because OHCA may not grant the request, entities should continue to calculate enough lead time into their closing timeline to complete the notice process.
For a copy of the regulations, please click here.
Reporter, Taylor Whitten, Sacramento, +1 916 321 4815, twhitten@kslaw.com.
King & Spalding Client Alert: FDA’s Latest Salvo in the Laboratory Developed Tests (LDT) Wars
On September 29, 2023, the Food & Drug Administration (FDA) published a long-awaited proposed rule on laboratory developed tests. The proposed rule shows that FDA is still asserting that it has statutory authority over all laboratory developed tests and has not significantly changed its thinking on laboratory developed tests since it issued draft guidance on the topic in 2014. The proposed rule is open for public comment through December 2, 2023. Read more about this proposed rule from King & Spalding’s Client Alert on this topic here.
King & Spalding Client Alert: DOJ “Safe Harbor Policy” Announcement Incentivizes Merger-Related Disclosures
On October 4, 2023, DOJ’s Deputy Attorney General Lisa Monaco announced a new “Mergers & Acquisitions Safe Harbor Policy” for companies that voluntarily self-disclose corporate criminal misconduct to DOJ. Under the new policy, companies that engage in a merger or acquisition and voluntarily and timely self-disclose criminal misconduct at the acquired company will receive a presumption of a criminal declination if they cooperate with DOJ’s ensuing investigation and “engage in requisite, timely and appropriate remediation, restitution, and disgorgement.” The announcement of the policy presents critical strategic and compliance considerations for companies that might participate on either side of a merger or acquisition, and reinforces that DOJ is paying close attention to potential liability associated with acquisitions of all shapes and sizes. Read more about the policy in King & Spalding’s Client Alert on the topic here.