Fifth Circuit Holds District Court Has Jurisdiction to Decide Repayment Amount Owed by HHS to Medicare Provider as an “Effectuation” of Prior Initial Overpayment Determination – On January 3, 2022, the U.S. Court of Appeals for the Fifth Circuit Court reversed the decision of the District Court for the Western District of Louisiana dismissing for lack of jurisdiction a Medicare provider’s suit seeking a determination of the repayment amount to the provider by HHS in connection with a prior initial determination that HHS erroneously recouped overpayment amounts from the provider. Applying the U.S. Supreme Court’s decision in Shalala v. Illinois Council on Long Term Care, Inc., 529 U.S. 1 (2000), the Fifth Circuit concluded that the district court had jurisdiction over the provider’s repayment suit where, as here, the suit is a continuation of the initial determination by the Medicare Appeals Council (MAC) that HHS had erroneously recouped overpayment amounts from the provider. The Fifth Circuit held that suits by Medicare providers seeking repayment of amounts erroneously recouped by HHS are reviewable by district courts under 42 U.S.C. 405(g) as continuous aspects of the initial, properly exhausted, administrative decision.
The Medicare provider in this case provided medical laboratory testing services to nursing homes and homebound Medicare beneficiaries. In 2014, a Medicare integrity contractor found that HHS had overpaid the Medicare provider by over $8 million, and the contractor started recouping the overpaid amount on behalf of HHS. The Medicare provider administratively appealed the contractor’s overpayment determination. Several years later, at the end of a lengthy administrative appeal process, the MAC issued a decision in favor of the provider and reversed the contractor’s initial overpayment determination. However, the MAC failed to specify the repayment amount owed by HHS to the provider based on the contractor’s erroneous overpayment finding. The provider filed a federal district court action, seeking repayment of the amount improperly recouped by HHS.
HHS moved to dismiss the provider’s suit for lack of jurisdiction, arguing, among other things, that the Medicare provider had not administratively exhausted its repayment claim. The district court agreed and dismissed the suit, reasoning that the provider’s action seeking to “effectuate” the repayment of recouped funds constituted a separate agency action that the provider must first administratively exhaust.
On appeal, the Fifth Circuit reversed. According to the Fifth Circuit, under the Supreme Court’s decision in Illinois Council, “certain ‘contentions’ relevant to the ‘action arising under the Medicare Act’ are reviewable by the courts, even if those ‘contentions’ themselves were not subject to a hearing.” Specifically, federal courts have jurisdiction to review “any statutory or constitutional contention that the agency does not, or cannot, decide.” HHS argued “effectuating” the repayment of recouped funds was a decision the agency could decide because the Medicare provider could seek redetermination of the agency’s decision. However, the Fifth Circuit rejected HHS’s argument noting that redetermination only applies to “initial determinations” and an “initial determination” is a decision regarding an individual’s entitlement to benefits. Quantifying the required repayment is “inextricably intertwined with the initial exhausted agency action,” and could only occur after the Appeals Council had reversed the overpayment decision (i.e., after reversing the initial determination). Therefore, there could be no redetermination and quantifying the amount HHS owed to the provider was a question HHS “[did] not, and cannot, decide.”
The Court also added, “it would be unconscionable to require a party to exhaust administrative remedies in order to prove that Medicare erroneously collected recoupment, and then to spend several more years of administrative appeals simply to determine the amount it is owed.”
The case is D&G Holdings, L.L.C. v. Becerra, No. 20-cv-30732, 2022 WL 18979 (5th Cir. Jan. 3, 2022). The full opinion is available here.
Reporter, Nicholas Kump, Sacramento, +1 916 321 4817, nkump@kslaw.com.
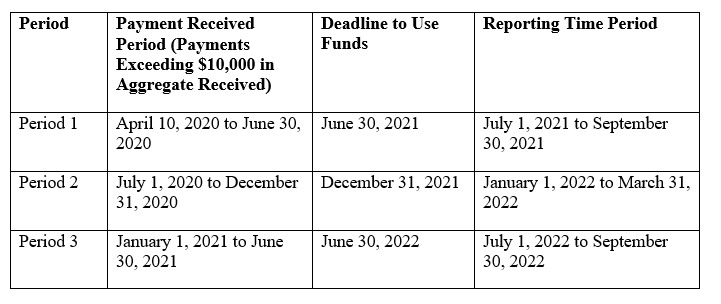
Provider Relief Fund Reporting Period 2 Now Open – The Provider Relief Fund (PRF) Reporting Portal opened for Reporting Period 2 on January 1, 2022. Recipients who received one or more General and/or Targeted PRF payments exceeding $10,000 in the aggregate from July 1, 2020 to December 31, 2020 must report on their use of funds in Reporting Period 2. The Reporting Portal for Reporting Period 2 will remain open through March 31, 2022 at 11:59 pm ET.
Period of Availability of Funds and Reporting Time Periods
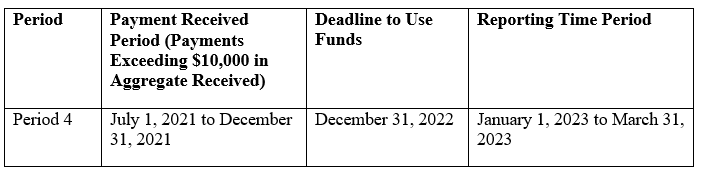
Providers are required to report on their use of funds in each Payment Received Period in which they received one or more payments exceeding, in the aggregate, $10,000, as indicated in the table below. Providers can only use payments for eligible expenses and lost revenues attributable to COVID-19 before the deadline corresponding to the relevant Payment Received Period. These deadlines are based on the date the payments are received (i.e., the deposit date for automated clearing house (ACH) payments or the check cashed date). Furthermore, reporting must be completed and submitted to HRSA by the last date of the relevant Reporting Time Period.
Reporting Period 2 Updates
If a recipient has previously reported, they may log into the Portal with their existing username, TIN, and password. (Note: New PRF Reporting Portal users must first register.) If applicable, the Reporting Portal will auto-populate previously entered data in certain fields, and recipients can edit and update any auto-populated fields. If changes are made to prepopulated data, once saved, the Portal cannot revert data back in case of error, and information must be manually re-entered.
It is important to remember that the Period of Availability for Reporting Period 2 payments overlaps with payments received in Reporting Period 1. Therefore, providers will need to show how payments were applied to expenses and lost revenues from Q1 2020 through Q4 of 2021. The expenses and lost revenues for Q3 2021 and Q4 2021 must not be duplicative of those included in the Reporting Period 1 report for Q1 2020 through Q2 2021. Furthermore, returning reporting entities may change the methodology for calculating lost revenues but must then use the new methodology to calculate lost revenues for the entire Reporting Period 2 timeframe. As a reminder, there are three options to calculate lost revenues:
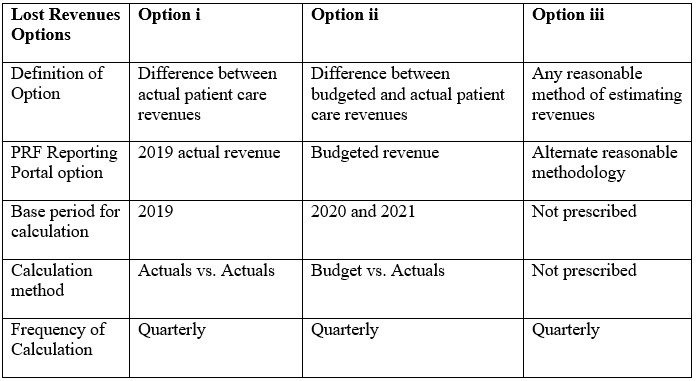
Updated HRSA guidance for Reporting Period 2 provides the information necessary for each option.
-
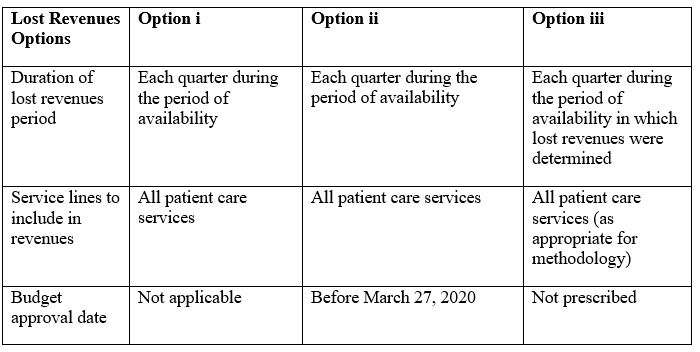
Option i: Difference between actual patient care revenues
-
Actuals for each quarter during the period of availability.
-
Actuals for 2019.
-
Option ii: Difference between budgeted and actual patient care revenues
-
Actuals for each quarter during Period of Availability.
-
Budgets for each quarter during the Period of Availability.
-
Copy of the budget approved before March 27, 2020.
-
Executive-level attestation.
-
Option iii: Any reasonable method of estimating revenues
-
Calculated lost revenues for each quarter during the Period of Availability.
-
A narrative document describing the methodology, including an explanation of why the methodology is reasonable for the circumstances, and a description establishing how lost revenues were attributable to coronavirus (as opposed to a loss caused by any other source).
-
A calculation of lost revenues attributable to coronavirus using the methodology described in the narrative document.
Finally, returning recipients may change previously reported financial information as part of the lost revenues calculation if there was a change to their patient care revenue since the Reporting Period 1 report was filed. If changes are made to previously submitted data, providers must write a justification for the change. For providers who reported in Reporting Period 1, the Reporting Portal will calculate remaining unused lost revenues that can be reimbursed by PRF payments received during future payment periods.
More information on Reporting Period 2, including updated guidance from HRSA, is available here.
Reporter, Ahsin Azim, Washington, D.C., +1 202 626 9262, aazim@kslaw.com.
OIG Publishes New Procedural Process for Advisory Opinions – On January 6, 2022, OIG issued a final rule (Final Rule) that will update the process and procedures that govern advisory opinions in early 2022. The Final Rule will be effective 30 days after its publication in the Federal Register (which is pending).
Historically, OIG has taken the position that it will not issue an advisory opinion when a similar or identical action or question is under investigation, or is the subject of a proceeding involving HHS, DOJ, or another governmental agency. This restriction was put in place to prevent OIG’s review from interfering with the investigatory or prosecutorial authority of other governmental agencies.
The Final Rule removes this restriction and expands OIG’s authority to review this type of conduct. OIG has determined that removing this restriction would allow it more flexibility in considering and issuing opinions while increasing transparency. The Final Rule mentions that the previous restriction prevented industry stakeholders from understanding how their conduct would be evaluated specifically under federal fraud and abuse authorities as other governmental agencies were not reviewing their conduct under this standard.
OIG also indicated that: (a) the existence of an active government investigation or other proceeding with respect to certain conduct could indicate that the conduct runs afoul of the federal anti-kickback statute or OIG’s administrative enforcement authorities and therefore subject to sanctions; and (b) conduct that is similar or identical to conduct that is otherwise under the review of the federal government may call for enforcement actions or sanctions.
The OIG’s Final Rule can be found here.
The Policy Statement can be found here.
Reporter, Kimberly Rai, New York, +1 212 556 2198, krai@kslaw.com.
CMS Releases Medicare Advantage and Part D Proposed Rule – On January 6, 2022, CMS published a proposed rule (Proposed Rule) which would revise Medicare Advantage (Part C) and Medicare Prescription Drug Benefit (Part D) regulations. CMS simultaneously released a fact sheet (Fact Sheet) stating that the Proposed Rule is intended to lower out-of-pocket Medicare Part D prescription drug costs and improve consumer protections, among other things. Notably, the Proposed Rule would revise Medicare Advantage and Part D regulations relating to marketing and communications, provider network adequacy requirements, and medical loss ratio reporting. Set forth below is a high-level summary of certain significant changes in the Proposed Rule.
-
Prescription Drug Costs. The Proposed Rule would require Part D plans to apply all price concessions received from network pharmacies to the price received at the point of sale when determining the negotiated drug price which is reported to CMS. The Fact Sheet states that CMS is proposing this change to target a practice by which Part D plans have entered into arrangements with pharmacies providing for discounts if the pharmacy fails to meet certain criteria, which results in plans reporting a negotiated price which is higher than the final payment to the pharmacies. The Fact Sheet states that revising the definition to require incorporating discounts will “reduce beneficiary out-of-pocket costs and improve price transparency and competition in the Part D program.”
-
Marketing. The Proposed Rule would implement new regulations which are applicable to certain third-party marketing organizations (TPMOs) which sell multiple Medicare Advantage and Part D products. TPMOs would be required to include certain disclaimers when marketing Medicare Advantage and Part D products. Any plan that does business with a TPMO would be subject to new oversight requirements to ensure that the TPMO adheres to any requirements applicable to the plan.
-
Network Adequacy. Applicants seeking to offer new Medicare Advantage plans would be required to demonstrate compliance with network adequacy standards as part of the application process for new and expanding service areas. CMS would give a credit of 10% toward meeting the proposed target established for the percentage of beneficiaries residing within published time and distance standards (used to measure network adequacy) prior to the start of the coverage year. After the coverage year begins, the credit would no longer apply, and the plan must be in full compliance. The Fact Sheet states that the credit is intended to avoid imposing a burdensome requirement for a plan to have a fully built-out network during the application process, which takes place almost a year in advance of the contract year.
-
Medical Loss Ratio (MLR) Reporting. The enhanced MLR reporting standards that were in effect from 2014–17 would be reinstated. Medicare Advantage and Part D plans would be required to report underlying cost and revenue information necessary for verifying the reported MLR and the amount of any remittance owed for failure to meet the minimum MLR of 85%. Medicare Advantage plans would also be required to report how much they spend on supplemental benefits not covered under traditional Medicare, such as dental and vision benefits.
-
Access During Disasters and Emergencies. Medicare Advantage regulations currently include special requirements for plans to cover services by non-contracted providers and waive gatekeeper referral requirements during emergencies, including during a public health emergency. The Proposed Rule would clarify that these special requirements will continue throughout any declared disaster or emergency period.
-
Plan Request Denials. The Proposed Rule would expand the list of reasons for which CMS can deny a new contract for a Medicare Advantage plan or Part D sponsor to include having a Star Rating of 2.5 or lower, filing for bankruptcy and having a number of compliance actions which exceeds a threshold to be established by CMS.
Comments on the Proposed Rule are due by March 7, 2022.
The Proposed Rule, Contract Year 2023 Policy and Technical Changes to the Medicare Advantage and Medicare Prescription Drug Benefit Programs, is available here. A CMS fact sheet summarizing the Proposed Rule is available here.
Reporter, J. Gardner Armsby, Atlanta, +1 404 572 2760, garmsby@kslaw.com.
COMPLIANCE COLUMN
King & Spalding Collecting Comments to Respond to OIG’s Request for Information on Modernizing its Publicly Available Resources - King & Spalding’s healthcare compliance practice will submit comments in response to OIG’s Request for Information (RFI) seeking feedback on how OIG could improve the usefulness, timeliness, accessibility, and usability of its publicly available resources, such as guidance, program integrity materials, publicly available data, and Advisory Opinions. King & Spalding will submit comments to OIG and has developed a brief, 5-minute survey to collect insight and feedback from clients and colleagues, available here. In addition, we would welcome the opportunity to discuss feedback directly, and you may reach out to Andi Bosshart if you would like to offer suggestions.
OIG acknowledged that many of its resources have not been updated in years. OIG seeks to improve both the effectiveness and the efficiency with which it makes materials available and seeks to make data and information available “in ways that are compatible with the technologies used by stakeholders.”
Specifically, the RFI offers stakeholders a mechanism to help OIG improve the usefulness, timeliness, accessibility, and usability of its resources by:
-
Providing insight into how they use OIG resources,
-
Identifying the successes and challenges with using OIG resources, and,
-
Suggesting other potential opportunities for OIG to provide information.
The RFI is organized by the various types of OIG resources (e.g. Advisory Opinions, Corporate Integrity Agreements (CIAs), Fraud Alerts, and Frequently Asked Questions (FAQs)). Respondents may elect to answer a series of broad questions posed by OIG covering the resources generally, or they may provide feedback regarding specific categories of OIG resources. Respondents are not required to respond to questions or provide feedback on every OIG resource. Responses to the RFI are due no later than January 31, 2022 and must be submitted electronically. OIG’s RFI is available here.
King & Spalding will submit comments to OIG and would appreciate insights or feedback shared by our clients and colleagues. For example, based on our experience using OIG resources, we plan to recommend that OIG categorize certain resources by topic or category. For instance, Advisory Opinions are currently listed by date of issuance. Similarly, CIAs are currently organized by the individual or entity’s name and OIG does not provide a streamlined way to identify CIAs by organization type (such as hospital, hospice, or physician group) or by characteristics of the CIA (such as including an arrangement’s review or compliance expert requirement).
As noted above, King & Spalding has created a survey to collect feedback, available here. In addition, you may reach out directly to Andi Bosshart if you would like to offer feedback or suggestions to be included in King & Spalding’s comment process.
Reporters, Andi Bosshart, Atlanta, +1 404 572 2657, abosshart@kslaw.com, Lauren S. Gennett, Atlanta, +1 404 572 3592, lgennett@kslaw.com.
ALSO IN THE NEWS
King & Spalding Webinar: 2022 Outlook for California Healthcare Providers – On January 18, at 12:00 pm PT, King & Spalding will be hosting a 90-minute webinar to provide an overview of a number of new legislative and health policy updates affecting California providers in 2022.
Topics will include the following:
-
updates to hospitals’ obligations to provide financial assistance and charity care;
-
significant changes to the Medi-Cal Program under CalAIM;
-
annual hospital equity reports that must analyze health status and access to care disparities and establish a plan to reduce those disparities;
-
the establishment of a California Health and Human Services Data Exchange Framework for sharing data between government agencies and providers; and
-
new requirements for SNF and LTC facilities.
The presenters include John Barnes, Kyle Gotchy, Vinay Kohli, and Taylor Whitten. To register for the event, click here.